
What underwear are you wearing right now? Do you know what color it is? Red, blue, pink, or some fun design? Do remember what is without looking at it?
This can either be a legitimate question, or perhaps a joke. Maybe even a fun post on Facebook or website that requires taking a quiz. It’s a question that can also get you sent to human resources or worse depending on who you ask! For the sake of this post, your underwear choice for the day is often the first conscious decision you will make to start your day (assuming you don’t have a variety of bath soaps or toothpastes to choose from).
Your day’s decision making will consist of some decisions that are largely inconsequential, like the underwear you choose to wear. A lot of the decisions you make will range from inconsequential to potentially life-changing. Of course, you can argue that choosing to take one route versus another to work had ultimately prevented a Final Destination-style event, but that goes well beyond the purpose of this post. So far the sake of simplicity, let’s assume that stopping to pick up food from a certain restaurant or taking a specific route is still largely inconsequential.
When I’m at work in St. Louis as a commuter without my family present, I have a very specific routine to start my day. It’s either a “workout day” or “off day,” where ideally this alternates every other day. If it’s a “workout day,” I will wake up usually around 6-7PM and take my pre-workout stack. I’ll browse the patient list and emergency department census to see how the swing shift is doing. If it’s super busy, I’ll start sooner. If it’s slow, I’ll take my time. Usually the pre-workout stack starts to hit at this point with the beta-alanine tingle throughout my body. I’ll workout for a bit and then have my post-workout shake. After the shake and post-workout stack, I’ll shower. After showering, I will choose my underwear for the evening. I usually don’t put much thought into this, and will randomly grab a pair from the clean pile. Honestly, I put a bit more effort into figuring out a colorful pair of scrubs to wear! Most people don’t wear scrubs to work, hence why this post is based on underwear.
My “off day” where I’m not working out will consist of me stopping for fast food prior to work. Depending on how busy it is, I will either get something from the most convenient locations to work consisting of Taco Bell, McDonald’s, Arby’s, or Chick-Fil-A. If it’s the weekend where it tends to be slower, I will venture out a little further and cross I-270, where I may get Panda Express or Lion’s Choice.
Assuming that I haven’t already started remotely from my apartment with patient care, the choice of underwear, scrubs, and food on a non-workout day are the largely inconsequential decisions that I will be making before actually getting to work.
By the time I arrive at the hospital and log into Epic, every single decision being made will now have an impact on the patient. Despite every single decision ultimately impacting the patient, you will still see them range from being inconsequential to having “life or death” ramifications.
Inconsequential and “always right”
Admitting patients to the hospital is reliant on admissions order sets. Every hospital has these. These are largely nursing orders to ensure the patient is appropriately cared for. Although vital, these are generally standardized depending on the patient disposition. For instance, a patient being admitted to the medical floor will have different monitoring parameters compared to a patient being admitted to the stepdown (more complicated) unit. ICU guidelines are mandated by state health departments and national accreditation organizations. Therefore assuming appropriate patient disposition, the basic admission orders are technically “always right.” Order sets can also offer basic medications to address commonly observed issues during the hospitalization. One of them is secondary insomnia, and melatonin is usually a popular first-line option since it’s harmless during a short-term stay and does not interact with other medications. I would call this inconsequential, and it can certainly save whomever is performing cross-cover at night some time.
And now there are consequences as decisions change colors from black to gray…
If the patient is going to a medical/surgical floor, they may or may not need telemetry. At this point, your medical decision making will start to have consequences. Figuring out the need for telemetry is not rocket science, and should be straight-forward. A patient is coming in for chest pain and you’re admitting for an “acute coronary syndrome (ACS) rule out?” Stick them on strict telemetry. Acute blood loss anemia due to an upper gastrointestinal bleed? Stick them on strict telemetry. A healthy 19 year old being admitted for a right lower extremity cellulitis with normal vitals and unremarkable ECG? There is no need for telemetry at this time. If the very same healthy 19 year old above suddenly becomes septic with hypotension, tachypnea, and probable tachycardia; then they would require telemetry at the very minimum. If they are sent to the stepdown unit or ICU, they would be on continuous cardiac monitoring.
Strictly black and white decisions… When they are right or blatantly wrong…
I really enjoyed the series “Sons of Anarchy.” It is a terrific modern-day adaptation of Shakespeare’s “Hamlet.” If there is one thing that “Sons of Anarchy” clearly isn’t, it’s a medical show. The medical aspect of the show is absolutely egregious. In season 1 episode 12, Dr. Tara Knowles, said to use oral vancomycin for someone’s wound because “this’ll kill anything.”
If you had a patient with a history of MRSA infection(s) coming in with cellulitis and you ended up ordering oral vancomycin for MRSA coverage, one of a few things can happen. You will receive an email from your superior(s) telling you about the improper use of vancomycin and use this as a very much needed educational moment. If the patient ended up with a poor outcome, then you will end up in front of the peer review committee. Or worse, you may end up in a court of law at the receiving end of a malpractice lawsuit.
Why? Oral vancomycin has only two specific purposes. Treatment of clostridioides difficile diarrhea/colitis and prevention of clostridioides difficile in an admitted patient with prior history currently receiving inpatient antibiotics. Oral vancomycin is not absorbed systemically, and therefore it would never be used any infection aside from clostridioides difficile. “Sons of Anarchy” managed to go a step further (if that’s even possible), and claiming “this’ll kill anything.” Wrong! It is a narrow-spectrum antibiotic that is only effective against gram-positive bacteria with MRSA being the primary indication. Therefore if you’re initiating broad-spectrum antibiotic therapy for let’s say cellulitis, you will accompany vancomycin with a broad-spectrum antibiotic that would cover for gram-negative bacteria (penicillin, cephalosporin, fluoroquinolone, carbapenem, etc). Therefore, if you have an otherwise healthy 20 year old lady being admitted for a “raging UTI” or septic ureteral stone resulting in sepsis, vancomycin is not something you would add since it’s highly unlikely that this is being caused by gram-positive enterococcus. Unless the patient has a prior history of enterococcus or had grown other weird gram-positive bacteria in their cultures, you wouldn’t use intravenous vancomycin. How about vancomycin monotherapy because “this’ll kill anything?” Not a chance! Unless the patient has a history of vancomycin-sensitive enterococcus infections. Oral vancomycin? No. Don’t even go there!
Intravenous versus oral vancomycin is the most glaring example of a huge error, especially since this was on the TV show. This was initially highlighted in my medical school pharmacology examination, where they specifically asked about clostridioides difficile treatment. Therefore anyone practicing hospital medicine should know the difference between the two formulations, and also not to prescribe oral vancomycin to finish a patient’s antibiotic course for cellulitis.
Some blatantly wrong things may not be as obvious or will pop up later. Let’s use the urinary tract infection in an otherwise healthy 20 year old again. Assuming no cephalosporin allergies, I am 99% certain that she would be started on ceftriaxone, the not-so-glamorous 3rd generation cephalosporin hero of hospital medicine. If this were a multiple choice question on a medical school exam or boards exam, ceftriaxone would be the correct choice. Now what happens if the urine culture grows something you weren’t expecting? Extended-spectrum beta-lactamase positive escherichia coli infection? Ceftriaxone is no good. You would need a carbapenem or a super fancy cephalosporins like cefepime-enmetazobactam or ceftazidime-avibactam (this will likely need to be ordered by an infectious diseases physician). Pseudomonas aeruginosa (wow, that’s a surprise)? You will need an anti-pseudomonal antibiotics such as cefepime, ceftazidime, or of course my personal favorite piperacillin/tazobactam.
As you can see with the last paragraph, a continued patient course can suddenly change direction depending on further imaging or lab studies. It’s important to stay on top of this, as what was once right now becomes wrong.
This finally helps transition us to what makes up a large portion of healthcare, the “grey area.”
Once decisions are no longer black and white… There is a massive grey area!
I would like to start this section by quoting my esteemed friend and colleague, Dr. Raj Singh. He once said something that really stuck with me: “If you do right by the patient, you can do no wrong.”
This is 100% true. I can’t stress this enough. This is the sole purpose of my job. It has 0% to do with me, and 100% to do with the patient. With that said, a large amount of my work is performed in the “grey area.” This is why I had years of education in medical school and then in residency prior to starting my career as an attending. But since the education is technically never-ending, I have been improving my skills and knowledge over the past few years of an attending physician.
Much of medicine is an art, and what I do may differ from an attending physician that sits just a few chairs away from me in the office.
One of the most obvious things behind my decision making process is my preference for penicillins over cephalosporins infections outside the urinary tract.

I bought this Ancef (cefazolin) tumbler a while back. But in all honesty, my favorite antibiotic is Zosyn (piperacillin/tazobactam). I love it for the incredibly broad antimicrobial coverage including pseudomonas aeruginosa and anaerobic bacteria. The pseudomonas coverage is valuable in many nursing home patients, especially when they have pneumonia. I like to follow along with my admissions when I’m able to, and the pneumonia pathogen panel will frequently come back positive for pseudomonas in this patient population. Zosyn also covers for aspiration, which is also quite common in elderly or debilitated patients. The hospitalist sitting a few desks from me might have a preference for cephalosporins, and might use cefepime or ceftazidime. There is no risght or wrong answer.
I also order additional imaging fairly frequently to better assess certain situations. Every now and then when I’m on the fence, I put the ball in the patient’s court and ask them if they would like further imaging or not. I have seen patients and families go one way or another.
Ultimately, my 10+ straight days at work consists of countless decisions being made for what I personally believe to be the best decisions for the patients. Some of them are black and white, whereas others are gray as seen in the next section.
When you enter the dark part of the massive grey area…
Prior to diving into this section, I would like to tell you about who I am, and two things that I am not!
I am…

I’m a physician that works as a nocturnist/hospitalist. That means I admit patients to the hospital and strictly work nights. It has been a few years since I have thankfully woken up prior to noon.
I am not…

I am not God (or Dr. Zoidberg for that matter per the above photo). Do not mistake my lack of ego (or God complex) as a lack of confidence. I live roughly 330 miles from Mercy Hospital South. Therefore, I am a random person living very far away that the patients and families will meet while they are having a really bad day or maybe worst day of their life. To say that I should personally control the destiny of someone I had just met and spoke to for a half hour instead of their spouse of 60 years is ludicrous. I do not think so highly of myself that someone who lives hundreds of miles away and has only known the patient for a few minutes should suddenly make life and death determinations. I can of course guide patients and families through difficult situations and conversations, but I am unable to make certain decisions by myself. I can’t make someone “full code” or another patient “DNR” because I feel like it and believe it’s what’s right. That’s not up to me. It’s up to the patient and the family.
I am not…

I am not a law enforcement officer. For any patient that is competent to make their own decisions, I can’t simply put them on a clinical hold or “arrest them” because they are refusing admission or any of the medical care. As long as the patient is competent and is not on a clinical hold (where they are unable to make their own decisions), they are free to make their own decisions regardless of how bad (according to us) they might be.
Now let’s enter passive God-mode…
You’re the doctor. You are admitting three patients. What would you choose as the most appropriate code status? These are based on real cases and patient decisions from my own experiences.
- A 28 year old gentleman with a past medical history of diabetes mellitus type 2 and essential hypertension presents with rectal pain. He is found to have a perirectal abscess. He is being admitted for a colorectal surgery consultation and intravenous antibiotics.
A. Full Code
B. DNR
C. Comfort Measures Only
2. A 100 year old lady with a past medical history of congestive heart failure and paroxysmal atrial fibrillation on Eliquis presents with shortness of breath. She is found to have bilateral effusions, pulmonary edema, and is in atrial fibrillation with rapid ventricular response. She is being admitted for a cardiology consult, diuresis, and rate control.
A. Full Code
B. DNR
C. Comfort Measures Only
3. A 42 year old lady with no medical history presents with left flank pain. She is found to have an obstructing 9mm ureteral stone with hydronephrosis. She also has an associated urinary tract infection as evidenced by her urinalysis. She is being admitted for a urology consult and lithotripsy.
A. Full Code
B. DNR
C. Comfort Measures Only
Alright, now let’s go through the answers!
For the first case of the 28 year old gentleman being admitted for a perirectal abscess, the patient chose answer A (Full Code). He is young and healthy and wishes to have everything done if something were to suddenly happen. This line of reasoning makes up the majority of cases involving healthy younger individuals where you wouldn’t even have to think twice.
For the second case of the 100 year old lady coming in for acute on chronic congestive heart failure and paroxysmal atrial fibrillation with rapid response, the patient chose answer A (Full Code).

The patient is already too old to play with Legos. When they tell you they want everything done, you say “are you sure?” You then walk them throughout the entire process of what cardiopulmonary resuscitation would entail. They still say “yes.” I kind of lied about the age for comedic effect due to the age range for Legos. But I have had a handful of patients just under 100 years old that were “full code.” Some of them ended up changing to DNR later in the hospital course though. I’m going to guess you personally would have chosen choice B (DNR) in this case.
For the third case of the 42 year old otherwise healthy lady coming in for a left ureteral stone, the patient chose choice B (DNR). This case stands out in my mind because her husband and daughters were in the room with her. When she said she would not want to be resuscitated, her daughter exclaimed “mom!” You could see the fear in her daughter’s face. I explained that this does not mean she would be in a vegetative state, but she still insisted. Her husband sat there and nodded. Her daughter was nearly on the verge of tears. I carefully documented everything we discussed in regard to the code status in the bottom of my HPI. Spoiler alert. She had the lithotripsy performed and was discharged the following morning. This didn’t end up as a tragedy worthy of national headlines. I’m sure you would have chosen A (Full Code), as this had taken me by complete surprise.

As you can see, every physician will act as a Demigod to a certain extent. Between the relatively 28 year old being admitted for a perirectal abscess and 100 year old being admitted for acute on chronic congestive heart failure and paroxysmal atrial fibrillation with rapid response, there is some point in your brain where there’s a red flag being raised. In an ideal world, the 28 year old would be “full code” and the 100 year old would be “DNR.” Also the 42 year old above should be “full code.” The 42 year old took me by surprise. But at what age would the 42 year old have to be in order to put in a “DNR” without batting an eye? What kind of medical conditions would the 42 year old have in order to put in a “DNR” without batting an eye? Whether you want to admit it or not, you are subconsciously thinking about the appropriate code status with every patient you see. It would be dangerous if you didn’t. What if the 28 year old intended to say they didn’t want to be kept in a vegetative state, and you ended up making them DNR without giving it a second thought? Since I started working with patients in any kind of capacity from day one in medical school, I have only met two patients that wished to be alive under any kind of circumstance. Two!
One of the most important lessons regarding code status was taught to me by my amazing colleague and friend Mara, who is one of the rapid response nurses and has been there since my first day as an attending. She said that it is a very difficult and important decision for patients and families to make their code status. If we suddenly try to push them into reversing it or going backward, it will make the patient and family believe that they have made the wrong decision.
I remember in residency when a patient started to decompensate and was DNR/DNI, there was the urge to call the family due to the “oh crap” moment in the hopes of having them make the patient full code, or at least amenable to endotracheal intubation. When I discussed this with Mara, she stated that we spend virtually all of our time trying to make the patient better, and that it becomes scary when suddenly we hit a massive roadblock. This is especially evident if the patient is DNI (no endotracheal intubation) or BiPAP. I have learned to have the difficult conversations, and to provide actual comfort care when the patient and family decided that this was the direction they wanted to go. In the end, one thing everyone deserves is a dignified death. In choosing to go with comfort measures, that is ultimately giving the patient and family full control of their destiny. I will do anything to keep that transition as comfortable as possible.
Healthcare Paternalism and the effect on patient autonomy
In medical school, we learned that one of the foundations of healthcare is patient autonomy. This means the patient is free to make their own decisions. We all practice paternalistic healthcare, up to a point. Generally speaking, when I admit a patient they will usually oblige with the medical treatment plan. After all, we are making what we believe to be the best decision(s) all to the benefit of the patient. Depending on the patient and level of their own medical knowledge, some will question the things they are getting. Do you know what I think about that? It’s great! It helps to build a team-like dynamic between the practitioner and patient/family. As I have mentioned earlier, sometimes I will ask them what they want to do when I’m on the fence. Sometimes patients may decline certain things, like imaging. This is, however, all on a scale. At one end, you have the patient that puts 100% full faith into the physician and will go ahead with all testing, imaging, and treatments for the duration of their admission. On the other end, you have the patient refusing everything but still technically admitted as well as those that leave the hospital against medical advice. There are a lot of patients that leave the emergency department against medical advice. We don’t hear about these patients as a hospitalist since they never make it that far. Every now and then we have someone with a change of heart, and decides to leave against medical advice once the admissions process was started.
Patients can leave against medical advice (AMA) for a variety of reasons. Some are much more serious than others. A patient coming in with a transient ischemic attack or syncopal episode refusing admission? The odds are in their favor. A patient coming in with chest pain with three completely negative Troponins refusing admission for a morning stress test? The odds are also in their favor. But this is also on a scale. On the other end you can have patients where leaving against medical advice has an incredibly high probability of resulting in death.
I remember one of the most surprising AMA stories, as the patient never even made it as far as our hospital. Since we have multiple specialists, we take transfers from a lot of surrounding hospitals that are either critical access or lack certain specialties. In order to improve my workflow, I will sometimes do a “pre-admission” on these patients. It’s a win-win for everyone involved. My colleagues are happy since it fills up an admission slot for me and they can take other patients from the emergency department. The patient’s nurse is happy since the orders will all be signed and held ready to go at the drop of a hat. Then I’m happy since I know exactly what I’m getting and have everything already set up for them. I do this mainly for patients that are at another Mercy facility so that I can add in my own orders and labs, effectively managing the patient at both ends. Very rarely I will do a pre-admission on a transfer center patient coming from a non-Mercy facility. I will mostly do this for something I find very interesting or if it’s a “slam dunk” case (during extended shifts or weekends when things are slower). If the patient ends up not coming to the facility, then I have to manually delete every single pre-admission order so the transfer center can close the encounter.
I like to roll the dice and decided to do so with what I imagined would be a “slam dunk” admission coming from an outside hospital on a combined swing-night shift. I was going off the information given by the transfer center. It was an elderly lady with minimal past medical history coming in to the outside hospital emergency department for chest pain. Three Troponin were performed, as is expected. The Troponin, however, were going up exponentially. The ECG did not show an ST-elevation myocardial infarction. She was given aspirin and started on a heparin drip. This was undoubtedly a slam dunk case for a non-ST elevation myocardial infarction, so I went ahead and did the entire pre-admission.
A couple hours later I received the most surprising Epic chat imaginable from the transfer center. They were asking me to delete the orders since the patient decided to go home against medical advice! I was in disbelief. As stated above, this was not a case of chest pain with three negative Troponins leaving against medical advice. This is a case of a patient going home when they are actively having a heart attack! The two most likely results are either: The patient passes away at home or develops new-onset congestive heart failure and presents back to the emergency department with shortness of breath and cardiogenic shock. I do not know what ended up happening though.
In this case, the emergency medicine physician is not a police officer. They do not have the authority to “arrest” her despite the fact that she is making an absolutely horrible decision. They can attempt to talk her into staying, and I’m certain that’s what happened. But in the end, patient autonomy must be respected. It’s one of the most important foundations of healthcare after all.
Recently I was reminded of my own experience of patient autonomy when I saw a post in an MS-DOS and early Windows gaming group on Facebook. Someone posted photos of Castle Adventure, which was the very first game I ever played on a computer. Where did our family get our very first PC? It was from my dad’s cousin, Zem. He lived in Minnesota and for a while was traveling between New York City and Minnesota by car. He would always stop at our house and it was always such a great time to spend time with him. There were lots of great childhood memories with him as well as when I got older. Unfortunately, he was diagnosed with stage 4 cancer while I was in medical school. He decided not to pursue treatment. On the other hand, I wished that he did especially since he was so close to the Mayo Clinic. Instead, he was able to travel back to the Ukraine to see his hometown. He then passed away peacefully on his own terms. I was lucky enough to see him when I traveled to Minnesota with my wife during the 4th year of medical school. He took us out for dinner. It was one of the most difficult dinners that I ever had. We talked and joked like usual. We talked about the past. He reminded me how I always admired his Volvo. There was one thing that was never mentioned though, and it was the cancer. He told us he was looking forward to seeing us again in the future. But that was the last time I would ever see him.

I miss him.
The giant 20 foot inflatable gorilla in front of the car dealership
Some of the most surprising decisions people make have been centered around the heart and cancer. There is usually a kicker though, and one of them is congestive heart failure. During residency in Arkansas, the majority of my patients had COPD. Now in St. Louis I see far more congestive heart failure. I typically see it in three forms. Acute congestive heart failure (CHF), which is either acute on chronic (pre-existing) or new-onset. This will typically present with shortness of breath (most common) and associated findings of pulmonary edema and pleural effusions. You also typically have edema in the abdomen and lower extremities. The edema below the diaphragm (without lung findings) is another variation of CHF exacerbation admissions, but is less common. Acute CHF is a complicated admission all by itself, and the complexity grows The majority of time I’ll actually see congestive heart failure is in the patient’s problem list. As long as there isn’t significant fluid overload from this, it would end up as “chronic diastolic congestive heart failure” (normal ejection fraction) or “chronic combined systolic & diastolic congestive heart failure” (reduced ejection fraction). It’s there. Be mindful of aggressive intravenous fluid management. Regardless, the heart is still a ticking time bomb and the patient can go into a fatal arrhythmia such as ventricular tachycardia or ventricular fibrillation at any time (the risk is higher with very low ejection fractions, hence many patients have implantable defibrillators). This is unfortunately what happens when many people suddenly collapse while at home or in public requiring CPR. This can happen in the hospital too, even when the patient is being treated for something entirely unrelated to the heart. Finally, you have “surprise congestive heart failure” admissions. This is when the patient presents for something that has nothing to do with a typical acute CHF admission such as dysuria due to a urinary tract infection. But upon careful examination of the vitals, you see the patient’s is hypoxic. You order a chest x-ray, and see the patient’s lungs are full of fluid. You then end up with an acute CHF admission even though something else had brought them to the hospital.
I definitely see a lot of congestive heart failure. When it’s a chronic problem not currently in exacerbation, it frequently becomes an afterthought. But in all actuality, it is a very serious life limiting condition.
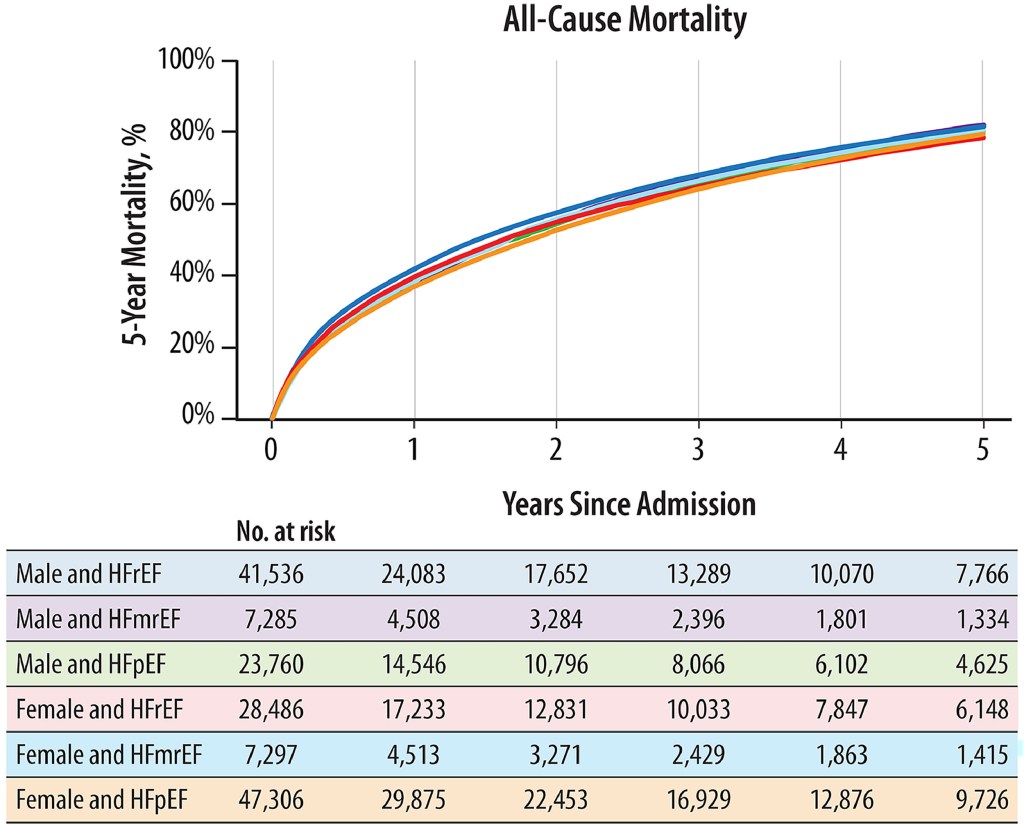
Above are some sobering statistics from the Journal of Cardiac Failure in 2024.
I remember a lecture from a well-respected cardiologist I know that emphasized how dismal these numbers are. This actually looks worse than many cancers, yet congestive heart failure is viewed very differently in the eyes of the public (and even healthcare workers) compared to metastatic cancer. That’s why congestive heart failure is often that “kicker” in the patient’s history, which can certainly sway decisions one way or another. It’s just like a giant 20 foot inflatable gorilla in front of a car dealership. How else will people in the street know there is a sale?

One of my greatest weaknesses is delivering a bad news or dismal prognosis to patients. I remember one time getting an admission from the emergency department for a patient that was just diagnosed with a widely metastatic cancer. The emergency medicine physician said it was good since I was getting this patient, since I have a “soft touch.” This can be a good or bad thing. But ultimately, I feel that it is my duty to give the patient the most realistic prognosis and information about their condition. It would be a disservice not to. Even when I have a patient with new-onset congestive heart failure, I try to be optimistic. Below is a clip from the movie “Manchester by the Sea,” which is a very good but emotionally heavy movie.
It is a pretty direct delivery above, for better or for worse. Congestive heart failure will feed into my final story at the end of this post.
The American Melting Pot
Our great nation is a nation of immigrants. Therefore in healthcare you will see people of all different cultures! I’m a first generation American Jew. My parents came to this country in 1979 from the former Soviet Union. Therefore I know the many quirks of other Eastern Europeans from the former Soviet Union. While in medical school, I have seen many patients that were from the same region and was able to speak Russian with them. Fun fact about St. Louis: It has the largest Bosnian population outside of Europe! There are some similarities in the quirks with Bosnian patients and then former Soviet patients. So I definitely understand where some of them are coming from. I won’t go into great details regarding this, but as a healthcare practitioner you should always be mindful of different cultures and how this can affect their different decisions. My colleague and closest friend at work, Aziz, is Bosnian. It’s great to have a brother that understands you and your culture, as we are both Eastern European.
Tying it all together with one final lesson
I have personally seen and heard of patients making decisions that really make us shake our heads. It can go both ways, whether they refuse all treatment or want to be very aggressive despite a terminal complication of cancer such as leptomeningeal carcinomatosis. Some of the big head scratchers have been in regard to severe coronary artery disease. Unfortunately, I am unable to tell you all about the largest head scratcher of all. This was not technically my patient, however, given the extreme specifics of the case it would certainly violate HIPAA. Just one other reason why I sometimes miss being at a teaching facility.
I remember going back and forth with a patient with severe coronary artery disease with stents and congestive heart failure regarding a coronary artery bypass. They refused it and were concerned about not surviving the surgery, despite the fact that they would die without the surgery. My colleague was bewildered with the constant volleying of questions and answers back and forth. The patient’s wishes were respected. He was trying to make sense of all this. I made it simple to understand. I told him that his choice of underwear for the day could be just as right or wrong as the patient’s decision of forgoing the bypass. Maybe he is wearing blue boxer briefs, but someone may find this to be the wrong decision as they would have expected red boxer briefs. Maybe just regular boxers? Therefore, although we may find their decision of forgoing a bypass as the clearly wrong decision. To the patient, they consider this right. Especially with the congestive heart failure “kicker” as a life limiting illness. We need to respect every single decision that a competent patient makes, regardless of what our professional and/or personal opinions may be. The same thing happens every time we put our underwear on to start the day. Maybe we got it just right? Or wrong? How about those cow-themed boxers? There’s really no right or wrong answer.


Leave a comment